Our Stories & Visions Gender in Black Immigrant Communities
Acknowledgments
We would like to extend our appreciation to those who helped us recruit Black immigrant women and femmes to participate in our research. This includes but is not limited to: BAJI staff and members, staff at other non-profit organizations, faith leaders, teachers, students, store owners, event planners, and those who simply helped us recruit by sharing our flyer with their families and friends.
Most importantly, we want to thank our incredible participants for sharing their sacred stories and visions with us. It truly took a village to make this project possible. We could not have done it without you.
The Black Alliance for Just Immigration (BAJI) educates and engages African American and Black immigrant communities to organize and advocate for racial, social and economic justice. Local BAJI Organizing Committees in New York, Georgia, California and Arizona build coalitions and initiate campaigns among communities to push for racial justice. At the local and regional level, BAJI provides training and technical assistance to partner organizations to develop leadership skills, works with faith communities to harness their prophetic voice, and initiates vibrant dialogues with African Americans and Black immigrants to discover more about race, our diverse identities, racism, migration and globalization.
Preferred Citation
Labiran, C. (2020). Our Stories and Visions: Gender in Black Immigrant Communities (Rep.). New York, NY: Black Alliance for Just Immigration.
Finally, we would like to thank Forward Together for their incredible support in bringing this report to life. Deep collaboration is possible when partners are value aligned and intimately listen to each other to inform the collective work.
Introduction
The trope that Black women and femmes are unwaveringly strong is killing us. This has become especially apparent at this present moment where we are attempting to survive a pandemic that is disproportionately impacting us while simultaneously being forced deeper into unpaid caregiving roles. From the experiences that Black women and femmes face in interpersonal relationships, to the discrimination we face in the workplace and at the hands of healthcare practitioners, our needs are oftentimes minimalized, or completely ignored. Even positive phrases like “Black girl magic” are weaponized and used to justify the lack of support that we are given. When we have the audacity to show signs of weakness, and assert that we are still human, we are labeled as overdramatic and emotional. We are denied the ability to be seen as complex beings, capable of embodying strength and weakness simultaneously.
As immigrants, we are forced into a space of non-belonging where we are made to feel like spectators in the U.S. Even in spaces with other Black women and femmes, the beauty of our differences can feel heavy. The discrimination we face based on our race, gender, immigration status, and other aspects of our identities has a cumulative toll on our minds, bodies and spirits.
Consequently, we are in search of spaces and relationships that simply allow us to be. We need restorative moments where we can allow our bodies to take a break from hypervigilance. Moments where safety is unthought of — it just is. Moments where we are held tightly by our communities and carried, if necessary.
We know, however, that our liberation cannot be fully actualized while our loved ones are incarcerated. We know that our liberation cannot be fully actualized when our families are separated at borders. We know that our liberation cannot be fully actualized while we are unable to fully explore our genders and sexualities. We know that our liberation cannot fully be actualized while we are unable to freely discuss our mental health and receive holistic, quality, affordable care.
BAJI’s Gender Justice program was launched because we believe our liberation is possible and that Black women and femmes are the people who will lead us there. This report was created to uplift stories and visions that we believe if listened to, and implemented, could radically transform the experiences of Black immigrant women and femmes in the U.S., and across the globe. Organizing spaces, including spaces that BAJI occupies, are not immune to harming Black women and femmes. As an organization we are committed to being introspective in our complicity and are working to internally and externally dismantle patriarchy and all forms of gender-based violence.
Background
While there are many areas of Black immigrant women and femmes’ lives that lack research, we have chosen to focus on mental health. Our research is in part motivated by the acculturation hypothesis — a phenomenon supported by research which indicates that the longer immigrants stay in the U.S., the more their mental health declines. Specifically, research shows that first generation (foreign-born) immigrants typically have better mental and physical health than immigrants who are U.S.-born.1 Additionally, foreign-born immigrants who move to the U.S. at an older age have a health advantage over those who move to the U.S. at a younger age. Interestingly, socioeconomic class does not appear to be a buffer as lower class first-generation immigrants have been shown to have better mental health outcomes than wealthier second-generation immigrants. Many refer to this initial advantage as the “immigrant paradox.”2
A recent study found that the acculturation hypothesis occurs within Black immigrant communities. In this study, researchers discovered that, in comparison to their U.S.-born counterparts, African and Caribbean immigrants who moved to the U.S. at age 13 or older had lower rates of anxiety and mood disorders.3 Conversely, those who moved to the U.S. before 13 years old had the same risk of developing anxiety and mood disorders as their U.S.-born counterparts. Undoubtedly, time of arrival is not the only factor that impacts the mental health of Black immigrants; research has shown that a wide variety of variables such as socioeconomic status, interpersonal relationships, social support, neighborhood context also have significant implications. Furthermore, beyond these factors that have been identified by research, we know that the various forms of systemic violence that Black immigrant women and femmes experience at the hands of actors such as law enforcement, medical practitioners and public benefits administrators also have adverse consequences on their mental health. The Black Women’s Blueprint report The Sexual Abuse to Maternal Mortality Pipeline demonstrates the link between weathering and mortality in the case of Black women.4 Specifically, they refer to research which found that “the stresses associated with living in a race-conscious society may lead to early health deterioration in Black women.”5
While some studies highlight that Black immigrants initially have better mental health than their U.S. counterparts, others show that the time when immigrants first come to the U.S. is the most stressful. This is especially true for people who are non-citizens and are oftentimes living in fear of detention or deportation. During this initial adjustment period, the mental health of Black immigrants can also be impacted by the lack of a support system, the lack of access to resources and language barriers.
Whether the stressors come earlier or later in the trajectory of peoples’ lives, it is important that we deepen our understanding of mental health for a variety of reasons including how high suicide rates are in Black immigrant communities and how violence is oftentimes the response to Black people in crisis. In 2018, Shukri-Ali, a 37-year-old Somali-American woman, was fatally shot after her family called 911 to get help for her. Cases like Shukri-Ali’s underscore how urgent it is that we implement alternatives to policing and are informed about the mental health challenges that people in our communities experience, so that we know how best to respond to their needs.
We are, however, not only interested in learning more about the mental health challenges that Black immigrant women and femmes experience, but also how they survive, and thrive against the odds. Research by Dr. Akinsulure-Smith on West African immigrants found that most respondents, despite experiencing high levels of psychological distress, relied on informal, culturally-informed coping strategies to better their mental health.6 Interestingly, only two participants in Dr. Akinsulure-Smith’s study reported going to therapy and they both had negative experiences. These findings are supported by Fanm Saj’s research on Sacred Healing Circles that found that only 10% of their sample utilized mental health or counseling services.7 The rest of their participants engaged in other healing strategies such as reiki, community building and crystal therapy. Consequently, this makes us curious to better understand the effectiveness of different forms of therapy. Furthermore, it makes us curious about the alternate avenues for healing that our people are tapping into.
Lastly, our research contains an imaginative component where we ask our participants to envision the kind of world they would create if they had no financial restrictions. In this section, we ask them to identify the role that their community can play in bringing this dream into fruition. We take these visions seriously and see them as contributing to a larger blueprint for the liberation of Black immigrant women and femmes.
Methodology
Recruitment
BAJI hired a Gender Justice Research Fellow in each of the following locations: New York City, Miami, Minneapolis and Los Angeles. They worked under the supervision of the Gender Justice Program Coordinator to assist with recruitment, conduct interviews, write transcriptions, and complete data entry.
BAJI’s graphic designer created a flyer to recruit participants. We strongly encouraged Black non-citizen, LGBTQ+ and formerly incarcerated individuals to participate. Furthermore, the flyer stated that all participants would be compensated $50 and that all interested individuals should email BAJI’s Gender Justice Program Coordinator. While the initial graphic called for women to participate in the study, we quickly realized this error and expanded our recruitment to include non-binary individuals. Our interviews took place in New York City, Miami, Minneapolis and Los Angeles — locations that have large and diverse Black immigrant communities. These areas also allowed us to have geographical representation from across the United States and coincided with locations where at least one BAJI staff person is based.
Locations: New York, Minneapolis, Southern California and Miami.
ALL PARTICIPANTS WILL BE COMPENSATED $50.
Contact: catherine@baji.org for more information.
In August 2019, we began sharing our recruitment flyer on social media. We also reached out to organizations and academic institutions in each of our target cities. BAJI staffers were instrumental in the recruitment process as they disseminated information on listservs, contacted BAJI members, and posted the flyer throughout their networks. After our Gender Justice Research Fellows came on board, our recruitment efforts shifted from being mainly online to face-to-face recruitment strategies. In Los Angeles, for example, BAJI was the official non-profit partner for Everyday People LA on October 6, 2019. Through this partnership, we were able to table at their event and, consequently, recruit participants for our research. In Miami, our fellow led Fanm Saj’s healing circle on October 10, 2019 where she was able to recruit additional interviewees. All fellows used snowball sampling as they asked their interviewees if they knew others who would be interested in participating.
Those who found out about our research online were prompted to contact BAJI’s Gender Justice Program Coordinator. In response, the Gender Justice Program Coordinator sent them a short Google form to fill out, which asked questions about their sexuality, age, ethnicity and location. In cities where we had more than 25 people interested in being interviewed we prioritized those who belonged to at least one of these groups:
- LGBTQ+
- Over 30 years old
- Not enrolled in an academic institution at the time of the study
- Lived in a borough, or an area that we did not have high representation
- Belongs to an ethnic group that we did not have high representation
Individuals who our Gender Justice Research Fellows recruited in person were added to a spreadsheet, so that the Gender Justice Program Coordinator could ensure that those who met the above criteria were prioritized.
Questionnaire Design
We created a questionnaire with 29 questions to assess the mental health and wellness of Black immigrant women and femmes. You can review the questionnaire in the Appendix. The first part of our questionnaire examines how the systemic violence that Black immigrant women and femmes experience impacts their mental health and wellness. We asked questions to examine their interpersonal relationships, interactions with law enforcement, public benefit administrators, and more. The latter part of the questionnaire assesses how Black immigrant women and femmes cope with these stressors and the healing mechanisms that they employ. Embedded in this section was a visionary component that allowed interviewees to tell us what they believe should be done to better the state of Black immigrant women in the U.S. and to inform us about the programming that they would create if they did not have financial limitations. Our questionnaire was reviewed and edited by BAJI staff people as well as teachers, academics, and therapists who have expertise in our areas of interest.
Interview Process
At the beginning of all interviews, our Gender Justice Research Fellows informed participants that the interview would be recorded before proceeding to turn on the voice recorder. After this, they read out the consent form as each interviewee read a written copy. If they agreed with the document, our fellows asked the interviewees to sign the consent form. At the end of the interview, participants were handed a gift card, mental health resource sheet and the contact information of the Gender Justice Program Coordinator. Three of our interviews required translation. In these cases, a BAJI staff person or family member translated to support the interviewer.

National Demographics
How did you hear about this research project?

BAJI Staff/Fellow 31.0%
Friend/Family/Coworker 23.8%
Listserv 9.5%
NGO 4.8%
Religious Institution 1.2%
Social Media 15.5%
Student Group 8.3%
Teacher/School 6.0%
How old are you?
Are you Employed?
Do you have any disabilities that you would be comfortable disclosing to us?
What is your gender?
Woman96.4%
Non-binary femme3.6%
What is your Sexuality?
What is your relationship status?

Of those who identified as single, 44.7% stated that they are happy with their relationship. 34% shared that they are neither happy nor unhappy. 8.5% shared that they are both happy and unhappy. There was no response from 10.6% of our single respondents. Only one participant (2.1%) shared that they are unhappy with being single.
39.1% of our respondents are in romantic relationships — 29% are dating and 10.1% are married. Of those that are in romantic relationships, 76.9% stated that they are happy. 10.3% shared that they are neither happy nor unhappy. 5.1% shared that they are happy and unhappy. An equal amount (5.1%) shared that they are unhappy. 2.6% gave no response.
Do you have children?
What Country Are You From?
(Note that some people identified with multiple countries)
Eritrea 1
Haiti 1
Liberia 1
Kenya 1
Trinidad and Tobago 2
Dominica 1
Ghana 3
Nigeria 1
Somalia 1
Jamaica 1
Guyana 1
Botswana 1
Colombia 1
Congo 1
Gambia 1
Guinea 1
Japan 1
Poland 1
Puerto Rico 1
Senegal 1
South Africa 1
Sierra Leone 1
St. Lucia 1
Sudan 1
Venezuela 1
Zambia 1
Zimbabwe 1
Are you a first or second generation immigrant?

Demographics by City
I know that my happiness is directly tied to love and feeling love and sharing love and like helping people, myself included, be better, um, better versions of themselves…I have learned that I need love. Like I’m that person. Like wow, amazing. And not just romantic love. I think people discount friend love and like familial love in a way that is unhealthy. Like I think everyone in my life is deeply important to me.
How old are you?
What is your Sexuality?
Heterosexual 63.0%
Bisexual 14.8%
Pansexual 11.1%
Queer 7.4%
Flexible 3.7%
What Country Are You From?
(Note that some people identified with multiple countries)
Antigua 1
Botswana 1
Congo 1
Dominica 2
Eritrea 1
Ethiopia 3
Gambia 1
Ghana 1
Guinea 1
Guyana 1
Haiti 1
Liberia 1
Nigeria 1
Senegal 1
Sierra Leone 1
Sudan 1
Togo 1
Trinidad 1
United States 1
Have you listened to Yolanda Adams…how could you not hear God in that voice if God exists? It’s in, you know, it’s in the voice of, you know, the African American….the African American woman’s throat. That’s where [God] exists.
How old are you?
What is your Sexuality?
Heterosexual 64%
Bisexual 12%
Queer 8%
Fluid 8%
Pansexual 4%
Unsure 4%
What Country Are You From?
(Note that some people identified with multiple countries)
United States 1
Bahamas 1
Dominican Republic 1
Ethiopia 1
Haiti 2
Jamaica 1
Kenya 1
Puerto Rico 1
St. Lucia 1
Trinidad and Tobago 1
Venezuela 1
We’re interconnected with each other and like the earth itself. Um, and that what we, everything that we do eventually has an impact on something else. Whether or not we think it is. So like dropping a cigarette butt might be the cigarette butt that flows into the Mississippi river. It makes it
toxic for everybody to not be able to drink. And so interconnectedness, kindness, generosity were the things that I decided to take from those [religions] rather than fear.
How old are you?
What is your Sexuality?
Heterosexual 84.6%
Fluid 3.8%
Bisexual 7.7%
Not Asked 3.8%
What Country Are You From?
(Note that some people identified with multiple countries)
United States 3
Ethiopia 9
Ghana 1
Haiti 2
Jamaica 1
Kenya 3
Liberia 5
Nigeria 1
Poland 1
Somalia 4
South Africa 1
Zimbabwe 1
Oh that butter, you know, the thing in the fridge actually has pins in it or like there’s sauce in that thing that’s marked oatmeal. Like, Oh, like we can relate to these things…about being first, second gen…or the cookie bin! The cookie bin. That red one! And it’s like why? Like why are these coins in here? I thought it was gonna be cookies. I don’t even know why I tricked myself like that. Of course it’s not going to cookies. When in all my years has it ever been?…Why is the plastic still on the furniture? It’s been years! It’s been years!…But anyway, that is what we bonded over.
How old are you?
What is your Sexuality?
Heterosexual 50%
Asexual 8.3%
Bisexual 8.3%
Queer 8.3%
No Response 25%
What Country Are You From?
(Note that some people identified with multiple countries)
Ethiopia 2
Ghana 2
United States 2
Colombia 1
Haiti 1
Japan 1
Kenya 1
Liberia 1
Nigeria 1
Zambia 1

Responsibilities, Support and Needs
CONTENT WARNING: political violence, natural disasters, food scarcity, homelessness, abandonment
My parents don’t drive. I take the train to school. Sometimes, I wish, I mean…I go to school in the Bronx…it takes two hours to get there. Sometimes I wish I could get a ride from my parents, and you know, call them, “mommy, you know, can you come pick me up?” And it’s cold outside, I’m going to work, and school can be tough because although they provide tutoring for certain classes, I’m not able to stay for tutoring because by the time I go to work and school it’s like 8:40pm. By the time I reach home, sometimes it’s like 10 o’clock or 11 o’clock. Sometimes I usually decide to stay in school to finish some of my work because I don’t have a laptop, so when I decide to stay and the library closes (it closes at 9:45 or 10 the latest) it usually takes me two hours to get to Brooklyn. So I reach Brooklyn by 1 am in the morning. It’s challenging and, and my parents sometimes don’t understand the challenges that I’m facing and they expect me to make doctor’s appointments and just everything else. I feel like everything is on my back right now…all of that is just pressure because now the future of the family, the financial future of the family, relies on my back.
WHEN I COMPARE IT TO BACK HOME, I was supported. I was cared for, I was provided for. But now, when I came here [to the United States], everything is…I have to do that. I have to provide for myself. I have to support myself. I have to do everything for myself. So when I compare that, um, that’s the big thing, it matures you, you grow fast, you know, you jump from, you know, being the child to a responsible adult right away when you come here because that circle of support is not there anymore. So, when I compare it, that’s the main thing I guess makes me…it’s like, um, what do you say?…um, the survival of the fittest everything about to survive. Yeah.
Responsibilities
Many of our participants stated that they are caregivers for their family members, which includes their younger siblings, parents, and grandparents. Some voiced that they are the “glue” to their families — the person who offers advice and connects people to each other. This sentiment appears to especially be true for first-born children and those who are made to assume that role due to the absence of an older sibling. We recognize these responsibilities as a reflection of the unfair burden that is placed on Black women and femmes who are disproportionately forced into unpaid caregiving roles.
Several of those who migrated to the U.S. independently expressed feeling like they had to “prove” that their families’ decision to support their migration was justified. In order to prove this, they oftentimes overwork themselves to succeed academically, professionally and financially. They noted that the lack of room that they are given to make mistakes, or to be human, has resulted in exhaustion, depression, and other adverse health outcomes. Our respondents shared that they feel compelled to prove that their families’ sacrifices are fruitful not only for their own sake, but also for their siblings and cousins back home, whom they are expected to open doors for.
There was great diversity in the responses shared by our interviewees as it relates to their families’ experiences back home. Many shared that their families are struggling due to political instability. Several of our respondents from Haiti shared that their families lives have been disrupted by political violence. A few respondents shared that their family members were either struggling with unemployment, or that they were unable to go to work due to Haiti’s political climate. Similar sentiments were shared by respondents with families in a range of countries including Ethiopia, Liberia and Somalia. One respondent shared that, at the time of the interview, teachers in Liberia were on strike because they had not been paid in four months. Beyond the high unemployment rates in these countries, our respondents also shared that their families struggle with access to healthcare and food. Many of our respondents with family members in the Caribbean and Puerto Rico shared that their families’ struggles are linked to recent hurricanes. For example, one of our respondents from Puerto Rico shared that her family is completely reliant on donations and that Puerto Rico is treated as though it is not part of the United States.
Of those who shared that their families back home are struggling, we asked if they believe their issues in the U.S. are incomparable to the issues their families abroad are experiencing. Our motivation for asking this question lies in the fact that we have heard from people who minimize their mental health concerns because they seem insignificant when compared to issues, such as food scarcity, that their families abroad are made to endure.
Do you believe that your issues are small in comparison to what people back home are experiencing?
No47.3%
Yes43.6%
Yes and No5.5%
No Response3.6%
We find it interesting that there is a close split between those who did not see their issues as significant when compared to their families and those who did. Some elaborated on their responses by sharing that they feel guilty that they have access to healthcare and food when their family back home does not. For this reason, they categorized mental health as insignificant in comparison to the challenges that their loved ones experience. Conversely, a few participants shared that they see their issues as equally important to the issues that their loved ones are experiencing despite the fact that they are different in nature.
Some of our participants, however, shared that their family abroad have no major struggles whatsoever. In speaking to such participants, we learned that financial stability was a major factor. For example, some of our participants shared that members of their family are in high ranked positions in either the army or government of their home countries, which has provided them with wealth and access to resources that the majority of people cannot obtain. Others shared that the source of their families financial stability is not related to their employment, but is instead due to remittances.
Beyond financial reasons, many shared that having community and a support system plays a major role in their family’s happiness. Through having people to rely on and to commune with, they are able to share responsibilities, avoid loneliness and have others care for them. Many participants contrasted the support that their families receive back home with their experience in the U.S. — a country that is largely individualistic.
Importantly, even in cases where participants stated that their family back home is doing well, that did not necessarily indicate that they had a good relationship with them. A few of our participants who are mixed race shared feeling abandoned or unsafe around their non-Black relatives:
Support Systems
Given the weight of these responsibilities, we were happy to hear that the majority of our participants feel that they have a support system in the U.S.
Do you have a support system in the U.S?
Yes95.2%
No4.8%
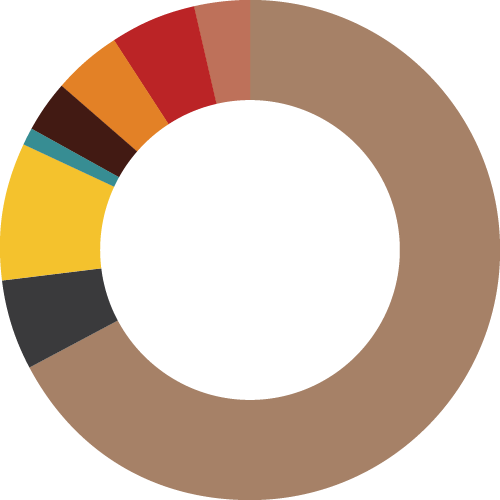
How strong is your support system in the U.S.?
Very Strong 66.7%
Strong 5.6%
Neither Strong Nor Weak 8.9%
Weak 1.1%
No Response 3.3%
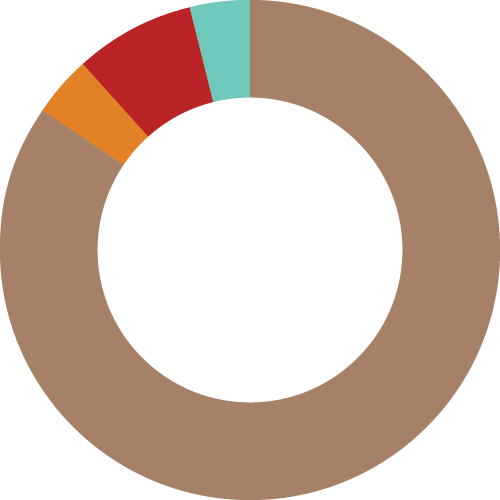
The image shown breaks down the strength of our participants’ support systems. 40.0% stated that their support system is “very strong.” 37.5% stated that their support system is “strong.”17.5% referred to their support system as “neither strong nor weak.” 2.5% referred to their support system as “weak.” 2.5% did not respond.
Furthermore, the majority of participants reported having a stronger support system in the U.S. than in their home country. We believe that there are a number of reasons for this including the fact that 40.2% of our participants were second-generation immigrants and many of those who were first-generation immigrants left their home country as children. Additionally, many of our participants stated that they have struggled to maintain familial relationships due to their inability to travel home.
While it appears to be a small number, we are dissatisfied with the fact that 4.8% of our participants do not have a support system at all. Later on in the report, we will share visions, recommendations, and resources that could help ensure that all of our people receive the support that they need.
Outside of formally asking respondents about their support systems, we also asked about their romantic relationships. Several respondents shared that their immigration status heavily influenced how they viewed their relationship. For example, some of our respondents, who are in the U.S. on student visas, voiced feeling stressed about the possibility of having to leave the country, and potentially their relationship, post-graduation. Consequently, they are forced to contemplate marrying their partner even though they would prefer for their relationship to progress at a slower pace.
While this was not the case in the above excerpt, we understand that due to restrictive immigration policies, many people are forced to marry their abusers. It should tell us a lot about the state of this country that after weighing their abusive relationships against the violence of deportation, many choose marriage.
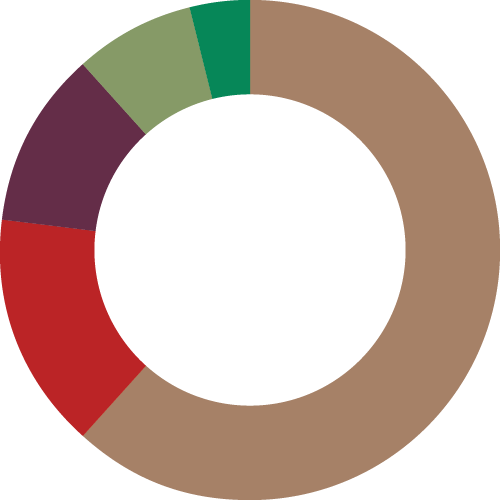
A further way we analyzed support was by asking participants if they have a space to be around other Black migrant women and femmes.
Do you have a place to be around other Black immigrant/femmes?
The image shown breaks down the percentage of participants who stated that they have a space to be around other Black immigrant women and femmes and those who did not. 75.9% stated that they have a space and 24.1% stated that they do not.
The benefits of such spaces are endless. Our interviewees voiced that these spaces were a place for them to rest. Through being in community, they do not have to code-switch, overthink their appearance, or spend an unwarranted amount of time explaining themselves. For once, they do not have to prioritize the needs of others over their own. In these spaces, they are able to center joy, laughter, and liberation in ways that they struggle to on a daily basis given the weight of their responsibilities. Furthermore, through sharing experiences with others in these spaces they are able to see that their stories are valid and their feelings are justified. Others elaborated on the emotional benefits of gathering with other Black immigrant women and femmes to state that they feel that such experiences are healing and have the ability to better their mental health. All of these benefits are reflected in the frequency in which Black immigrant women and femmes surround themselves with people of similar identities.
How often do you attend spaces with Black immigrant women and femmes?
Very Often 39.7%
Often 36.5%
Sometimes 17.5%
Rarely 6.3%
Government Benefits
My baby was five months old, I gave him to my sister so I could work in the evenings. Housekeeping was my first job…Five months. My son was five months old. And I asked my sister to babysit my kids and I used to work five hours. And my husband…he used to work in the airport. So we like to work. We work very hard.
But a lot of them…my country people, my community, we work very hard. We work very hard. Even we are ashamed to take like food stamps. All my family, we never get food stamps. Even when I came, they said you can get money. I told them no, I don’t need money if I get insurance. Because I used to stay with my sister in a two-bedroom. Maybe we are five or six people. I used to stay with them instead of taking government money.
When I was a kid we would go to get welfare or go on these long lines, you know, for government assistance. And I would be there for my mom to translate, or help her with her documents. I’d see the way the social workers used to talk to my mom, it was one of the reasons that I went into social work before my accident.

Beyond the support that Black immigrant women and femmes are provided by their loved ones and communities, we also wanted to know if our participants receive government benefits. In asking this, we aimed to assess people’s experiences from the moment they enroll to when they are ready to utilize said benefits. Overwhelmingly, our respondents shared that the enrollment process was tedious, bureaucratic and oftentimes involved going to several offices in different locations across the city. Additionally, several respondents described the customer service that they experienced within these offices as abrasive and described having to advocate for their parents in these spaces. This finding is supported by research conducted by the Urban Justice Center on Supplemental Nutrition Assistance Program (SNAP) and Public Assistance (PA) recipients. In their study, 34% of their respondents reported that Human Resource Administrators “always” or “often” spoke to them in a disrespectful manner. Another 33% reported that they “sometimes” received this mistreatment.8 In our study, several participants described how they became ineligible for benefits like Medicaid due to a salary increase, despite still having a need for support.
Unmet Needs
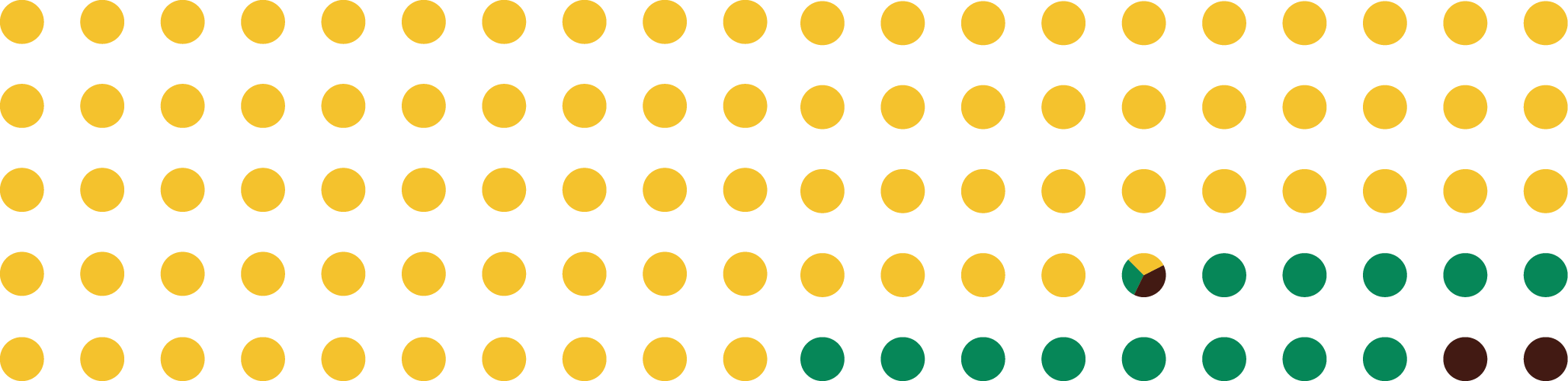
Given this lack of support, we asked participants if they have any unmet needs at the moment such as housing, clothing, or food.
Do you have any needs at the moment?

The image shown breaks down the percentage of participants who stated that they had unmet needs and those that said they do not. 50.6% stated that they have unmet needs and 49.4% stated that they do not.
Our needs assessment highlights widespread governmental failures: Why are so many people looking for affordable housing while, as of 2018, 250,000 rental apartments sit vacant in cities like NYC?9 The issue is not a shortage of resources, but instead how unfairly they are distributed. Consequently, our needs assessment highlights the need for community-based support and for an adoption of for us, by us strategies.
In sum, it is clear that the unmet needs and responsibilities that many Black immigrant women and femmes have outweighs the support that they are given. Given this imbalance, the concept of self-care becomes harder to actualize.
Expectations vs Reality
Importantly, such recollections point out that while there are material expectations, the expectation of social support is the most significant.
Confronting Discrimination in Schools and the Workplace
CONTENT WARNING: criminalization, Islamophobia, poverty, bullying, anti-Semitism
Many of our participants shared that they have experienced discrimination based on their race and gender in school and the workplace. Regardless of the location, their responses illustrated how heavily policed the bodies of Black women and femmes are in professional settings. From passing through metal detectors to enter school to being told that natural hair styles like braids, afros and dreadlocks are unprofessional, Black women and femmes are subjected to constant surveillance and are made to question if they truly have ownership over their bodies. Beyond making people feel as if their bodies are threats, we recognize the assumed criminality of screening Black students as one of the destructive links in the school to prison pipeline. Black immigrant Muslim women and femmes face a unique set of challenges as they oftentimes have to fight for the right to pray during the work or school day and the right to wear a hijab.
Black immigrants who have limited proficiency in English struggle to navigate professional settings with little to no guidance. Not only does this make their experience extremely isolating and confusing, it can also have terrible consequences on their
mental and physical health:
However, it is not only immigrants who have limited proficiency in English that are overworked. Several of our participants shared how they and their parents are wired to overwork even when it is unnecessary:
The unhealthy work ethic that Black immigrants are forced to adopt becomes internalized and makes them fearful of resting given that rest is oftentimes conflated with laziness. Capitalism is destructive and forces Black immigrants to feel as if they have to pay for their right to be in this country with the deterioration of their bodies.
Not only are Black immigrants grossly overworked, they are also chronically underpaid. In 2013, the median annual salary for Black immigrants was $43,800 — which is nearly $8000 less than the median annual salary for American households and over $4000 less than the median annual salary of other U.S. immigrants.10 Consequently, one in five Black immigrants live under the poverty line.11
In a country that criminalizes poverty, poor Black immigrants are left vulnerable to incarceration, deportation, and are unable to access lifesaving goods and services. Consequently, work in itself is not enough to provide Black immigrants with security. Black immigrants need safe workspaces that pay them a living wage and provide them with comprehensive benefit plans that meet their needs.
In schools, many Black immigrants are subjected to verbal abuse and are bullied by their peers, teachers, and administrators:
Also, umm in high school I was bullied because I was Haitian and I had an accent. So it impacted me so much that I started to stutter. My stuttering problem was so bad that my professor wrote me a recommendation letter to go to speech therapy. So I went and got speech therapy…Mentally you start questioning yourself, start doubting yourself. That can happen. Doubt yourself, question yourself. You might fall into depression just because you realize that you may not be enough.
I was a really confident little girl, very confident little girl, didn’t, didn’t know who I was in the world…I had experienced some things. My first time experiencing racism, it was being told I couldn’t swing on the tire swing with the other girls, I had to push it because I was Black, but I didn’t know what that meant. I was like, all right, but that’s crazy, but okay, but I’m a good pusher, so fine. So I pushed that tire swing…I was like, I know I’m strong, whatever. But then I was like, mom! And then she was like…that’s racism. Let’s discuss. She was luckily a TA, a teacher assistant, at that time. Let’s just say she discussed it with the other girl, too. And we came out friends ’cause mom was like, this little girl learned things in her home. It’s not you. It’s from her home. My mom was a teacher’s assistant for like one year and that was the year I was in that space. So luckily my mom was on hand ’cause I would not have told her if she were not there.
Several of our interviewees shared that other Black students called them “African booty scratcher” — a derogatory phrase commonly used in the U.S. to compare Black immigrants to primates.
In other cases, our interviewees shared that other Black students created, or helped spread, rumors about them. They expected that there would be greater solidarity between Black students from the U.S. and Black immigrants. Unfortunately, they were made to understand how harmful, anti-Black stereotypes, which were created and perpetuated by white people, had been internalized by their classmates.
Undoubtedly, these sentiments emphasized their feelings of isolation within the U.S. At BAJI, our core mission is to facilitate healing between all Black people. It is clear that we are stronger together and that we need each other to survive.
It is crucial to note, however, that it is not only students who are negatively impacted by discrimination in schools, it is also their parents. Several of our interviewees shared that the first time that they experienced racism it was through the mistreatment of their children:
Outside of the verbal abuse Black immigrants experience while in school, the institutions that many of them attend are also chronically underfunded:
This testimony is supported by research which found that predominately non-white school districts receive $23 billion less than school districts that predominately white. 12
Given the degree of mistreatment that Black immigrants experience in schools, they have to find ways to survive the system. From forming cultural and identity-based student groups to forming peer-to-peer support groups, Black immigrants find innovative ways to care for each other amid adversity. Another way that they protect their mental health is by choosing to physically segregate from non-Black students. Through being in all-Black spaces, they do not have to take on the labor of explaining their words, appearance, or behaviors to non-Black students. Furthermore, in these spaces they can be their whole selves without the unwanted pressure of assimilation.
Criminalization
CONTENT WARNING: ICE raids, police, CPS, detention, deportation, child abuse, sexual assault
We asked our participants how they feel when they hear about ICE raids, detention centers, deportation, and anti-immigrant rhetoric or policies. The majority of our participants expressed anger, frustration and disgust with regards to the mistreatment of Black immigrants. In particular, they were horrified by the images and stories of families being separated at the U.S.–Mexico border and throughout the states. Some of our participants who are documented shared that they live in the fear that their status could be taken away at any time. This fear makes them scared to watch the news, drive, go to the hospital, or even leave their houses. Others who are documented shared feeling afraid for their undocumented loved ones.
As they elaborated on their emotions, some of our participants shared that they find it deeply problematic that billions of dollars are poured into the destruction of Black immigrant lives instead of into underfunded sectors like the arts and education. Our participants also voiced concern about the erasure of Black immigrants in conversations on immigration. This invisibility makes their mistreatment even more horrific as it means that their stories are rarely reported and justice is rarely served. Their stories underscored the importance of solidarity between all Black people — regardless of whether they are immigrants and or not. It is crucial that we amplify each other’s stories and work to defend and protect each other.
We asked our participants how they feel when they hear about ICE raids, detention centers, deportation, and anti-immigrant rhetoric or policies. The majority of our participants expressed feeling anger, frustration and disgust with regards to the mistreatment of Black immigrants. In particular, they were horrified by the images and stories of families being separated at the U.S—Mexico border and throughout the states. Some of our participants who are documented shared that they live in the fear that their status could be taken away at any time. This fear makes them scared to watch the news, drive, go to the hospital, or even leave their houses. Others who are documented shared feeling afraid for their undocumented loved ones.
As they elaborated on their emotions, some of our participants shared that they find it deeply problematic that billions of dollars are poured into the destruction of Black immigrant lives instead of into underfunded sectors like the arts and education. Our participants also voiced concern about the erasure of Black immigrants in conversations on immigration. This invisibility makes their mistreatment even more horrific as it means that their stories are rarely reported and justice is rarely served. Their stories underscored the importance of solidarity between all Black people — regardless of whether they are immigrants and or not. It is crucial that we amplify each other’s stories and work to defend and protect each other.
Additionally, our interviewees opposed the idea that anti-immigrant policies started with the Trump administration. They detailed the fear that they lived under before and during the Obama administration. In other cases, despite knowing the steps that BAJI is taking to keep interviews confidential, some participants did not want to elaborate on how they feel about ICE out of fear that they could be deported.
One participant shared that after waiting two years to have status in the U.S., that she is considering leaving the country:
Another participant shared that they are more fearful of the police than they are of ICE. They expanded on their comment by sharing that they know that both agencies collaborate and that if they are brutalized and jailed at the hands of the police they know that they will also be handed over to ICE and potentially deported.
Sexual Assault and Harrassment
CONTENT WARNING: sexual assault, sexual harassment, child abuse
Have you experienced sexual assault or harassment?
While their research does not focus on Black immigrants specifically, findings from Black Women’s Blueprint’s Truth and Reconciliation Commission Report revealed that 70% of their participants had been sexually assaulted by the age of 18.13 Furthermore, their results showed that the average age that their participants first experienced sexual assault was 5 years old.14 Such statistics paint a horrific picture of the mistreatment of Black women and femmes — a mistreatment that stems from early childhood and haunts many of them throughout their lives.
Many Black immigrant women and femmes experience sexual assault before they arrive in the United States and are unable to access the healing and justice that they deserve after they migrate:
Unfortunately, many Black immigrant women and femmes, including those who were sexually assaulted in their home countries, are sexually assaulted on their way to the U.S. and while they live here. Disturbingly, several of our participants shared that they were sexually assaulted by a faith leader and that members of the congregation, including their family members, attempted to cover the incident up. Such experiences make it impossible for places of worship to be seen as sanctuaries. Instead, they become sites of trauma, betrayal and non-belonging for many Black immigrants.
Beyond the implications on faith, many Black immigrant women and femmes who experience sexual assault, or harassment are made to re-examine their politics as they seek justice and holistic healing. Specifically, in our research we heard from people who did not want to report sexual assault to the police but instead desired that their perpetrators hold themselves accountable for their actions:
Such testimonies highlight the need to expand upon community-based, survivor-centered accountability processes. We share some of these in Resources.
Religious and Spiritual Practices
Most of our respondents identify with a spiritual practice, or religion. For many of them, however, the religion or spiritual practice that they observe is not the same as the one that they were raised under. We found that people learned about their current faith practice through mediums like traveling, their grandparents, or college classes. For those who stated that they still practice the same religion that they were raised under, many had caveats. For example, many Christians stated that they no longer practice Christianity in the way that they did under the influence of their parents. Notably, many shared that they do not go to church given the violence that the church, as an institution, has enacted on Black lives.
Do you identify with a religion or spiritual practice?

Additionally, silencing of mental health concerns was repeatedly listed as a form of violence that the church exercises:
I just knew that I was having symptoms of deep sadness, anxiety, all of these things. But you couldn’t talk about that, you just had to pray about it. All the time, just pray about it. And I really think that as I got older…yes, pray about it. But also get the support and help that you need and don’t ignore it. And I don’t think that is something that is taken seriously in the church yet. That you can simultaneously pray about it, go to church for it, and also get…see a provider, see a mental health specialist. And it is sad because I know there are people in the church who are dealing with the same things and feel they can’t talk about it or put that label on it, because they will be seen as less than. So I have, I have issues with the church. Not only directly about the topic of mental health, but topics related to the injustices that we are seeing around the world. That makes my blood boil, seeing the church ignore it. Seeing the church support the president and the rhetoric that we hear each day. And I think being silent about it is supporting it too.
I’m the kind of person that wants to fight so that other people don’t have the same experiences as me. And if I were to follow the religion I grew up in, it would make me not fight. It would make me stay in the same spot and just keep praying that things would change.

Conversely, others noted that their churches are predominantly composed of, and in some cases led by, Black immigrants. In these cases, they believe that their church has the capacity to bring people together to create solutions for the issues that impact their mental health. Beyond gathering people, others identified critical resources that they have been able to access through going to church:
We believe that religious institutions are most instrumental when they work not only to ground their congregation in faith but when they also strive to meet the needs of their communities. Through forming support networks, religious institutions have the capacity to provide housing, food, clothing, childcare, healthcare, legal services, and more to their congregations and surrounding communities.
Many of our participants shared that while they do not have a formal religious practice, they have developed a deep sense of spirituality. They elaborated on their response to share that they have been looking back to the Indigenous spiritualities practiced in their home countries for guidance and grounding. It must be said, however, that making the shift from the religion that their parents practice to an exploration of what their ancestors observed does not come without its challenges. Some participants shared that they knowingly or unknowingly combine different faith practices, astrology, science and other forms of knowing to form their own unique spiritual practice. A few participants shared that they were demonized, marginalized and isolated for practicing faiths such as Vodun and Yoruba religion:
Experiences with Healthcare Practitioners
CONTENT WARNING: illness, disease, intergenerational trauma, physical abuse, child abuse, ageism, maternal mortality, fatphobia
Experiences with Therapists
And I mentioned this earlier, there’s like situational and then there’s like chronic. Yeah. So you know, I struggled for example, [with] like chronic, like back pain and it has flares and sometimes I’m like perfectly fine, but it’s always there. Um, and then I think that mental health too, like sometimes I just have really good times where it’s just like, I’m fine. Like, I don’t need therapy as much. I’m doing well and then something will happen and they’ll go about. And then there are people who are just like, they just have something happen that they do have like a situational period where they’re very depressed, like a death or something like that or something happens and they get really, really anxious. But it’s something that’s very situational and for other people it’s like, chronic.
And there’s so much research that has gone into mental health issues and struggles and you know, like the chemical imbalances in your brain, what’s going on with your dopamine and serotonin or whatever. But it’s deeper than just being like, I want to be happy. Of course most people want to be happy, like it’s a human desire. But achieving that happiness is multifactorial. And I think people just see the material part of it and that’s what they impart on their kids.
It is harder for people to find a good therapist than to be in a romantic relationship.

We don’t really do therapy. I think the first therapist in Haiti…clinic opened 2017? I mean the very first. The number one. And we are a country that has been in existence for…here we are celebrating our hundreds of years of independence and you are telling me this is the first therapist? How backwards right? But that is not what you did. You went to voodooism. Or you went to God. Or you did both, if you were wealthy enough to afford both. But therapy wasn’t a thing. So if it is not part of your culture, why would you do it? I think culture blocks it, I guess.
Throughout this section and report, we use the word therapy not to homogenize the field, but as an umbrella term for the various forms of therapy that exist. Some types of therapy include: cognitive behavioral therapy (CBT), art therapy and mindfulness-based cognitive therapy (MBCT).
have you ever gone to counseling/therapy?

Beyond the negative experiences that they have had personally, we asked participants if they believed that there are boundaries that prevent Black immigrant women and femmes from accessing therapy. Unsurprisingly, the overwhelming response was that there are plenty of boundaries that reduce the feasibility of therapy. One of the largest boundaries is cost. Those who have health insurance shared that their plan does not cover enough of the copay to make therapy affordable. Whereas, others shared that their plan did not cover therapy at all or that it did not cover the Black woman therapist that they desired to see.
Outside of cost, others shared that stigma, as projected by their cultures and families, was a large obstacle. Many shared that within their cultures the concept of mental health either “does not exist” or that it is invisibilized. Consequently, if they mention the desire to speak to a therapist they would be seen as a disgrace.
Interestingly, some participants shared that while their parents do not have the language to discuss mental health in the clinical, Western sense, they would use other words to describe their mental health:
Whether verbalized or not, we believe that the majority of our participants deeply desire to have intergenerational conversations about therapy with their families and communities. Our participants were concerned that their parents and grandparents who have experienced wars, colonialism, racism, sexism and other forms of oppression, declare that they have no trauma to unpack. Not only can these bottled up emotions adversely impact the person that harbors them, they can also manifest as intergenerational trauma. Consequently, it is important that elders are not forgotten in conversations about mental health and that we continue to find culturally competent ways to explain the importance of therapy and other forms of healing to them. As the quotes above indicate, many of our loved ones are eager to grow. Equally, it is also important that we are open and ready to receive the wisdom that they have as it pertains to wellness. Regardless of age or experience, we can all assume the role of both teacher and student.
I was talking to a couple of my friends and we were talking about the idea of whopping children and like the idea…it’s abuse, right? But we’ve been told that like this is how we discipline children and we’ve like accepted it in a way that it’s, it’s normalized that culture. But like if you went to talk to a therapist, if you had went to talk to like someone in the medical field, they would just associate it with abuse. And I think that abuse is also what we’ve learned from, like, colonization, with people coming on our land and the only way they wanted to discipline us was abuse. So it would go their way. And that’s what we’ve had to learn with each other.
I would write in my diary about how they didn’t get it…and I just wrote about how sad and depressed I was. Some days I’d wish I could just step in front of a truck and have the truck kill me like— I would write stuff like that. It was so bad, and they read it. And it was like I don’t think they got it, because what they told me in response to me wanting to get run over by a truck was just like, they said um *cough* if that happened to you, they were like if that happened to you, how would it look on us?

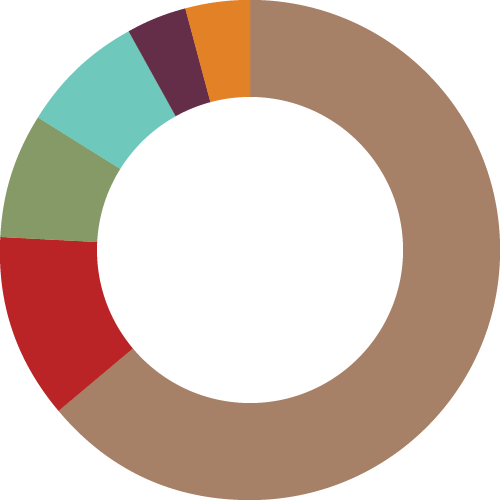
Experiences with Medical Practitioners
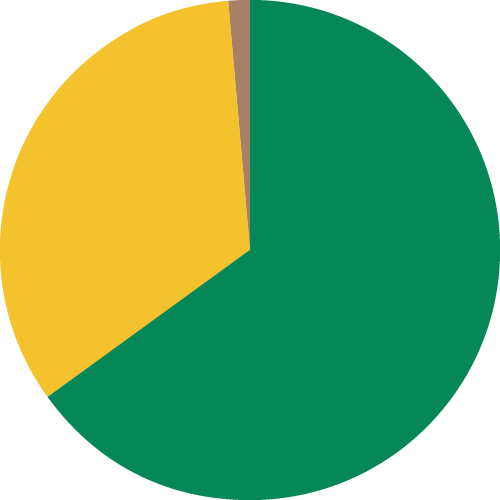
how would you describe your experiences with medical practioners in the U.S.?
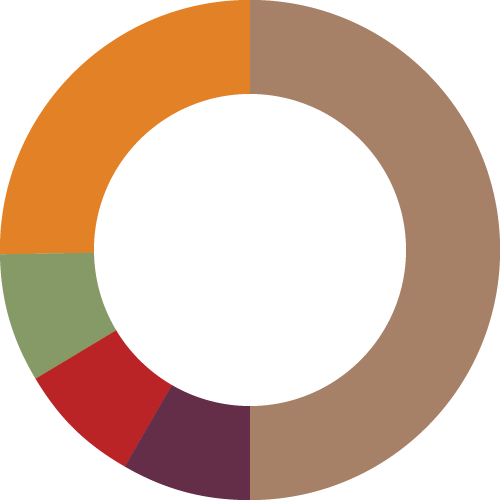
The image shown is of a pie-chart that describes the kinds of experiences that our participants have had with medical practitioners in the United States. 37.3% said that they have had bad experiences with medical practitioners. 25.3% said that they have had good experiences. 30.1% said that they have had both good and bad experiences. 4.8% shared that their experiences are neither good nor bad. One participant (1.2%) shared that they do not go to the doctor. One person (1.2%) did not respond.
The goal of the pie-chart is to present the general sentiments that our participants have towards their medical experiences in the U.S. However, we recognize that classifying things as simply “good” or “bad” is reductionist and does not capture the fullness of their experiences. Below we will delve further into the explanations which led us to categorize their experiences in the way that we did above.
The majority of our participants shared that they are dissatisfied with the medical care that they have experienced in the U.S. They shared stories of how they have been silenced, ignored, and touched without consent in doctors’ offices. Several of our participants identified that, due to their race, gender, and immigration status, their complaints were minimalized. Furthermore, they shared that within the medical field, Black people are treated as if they have higher pain thresholds than others. This widespread form of racism has been supported extensively by research.15 Additionally, several young people shared that their doctors used age to dismiss the severity of the concerns. This reveals the dire consequences of ageism that forces young people to advocate for themselves. Examples of such advocacy ranged from telling the doctor what prescription they need (based on prior usage) to pretending like they had family members in the waiting room so that they receive a timely and adequate response.
Cost was identified as a major barrier to healthcare. Some participants, especially those who are undocumented, shared that they rarely visit doctors due to the financial burden. One participant shared that she had to wait until after she married her partner, who is a U.S. citizen, before she could receive the care that she urgently needed under his insurance. Others shared that due to financial barriers, they try not to see doctors and instead try to heal themselves with herbal remedies.
Another barrier is the lack of language accessibility which leaves those who are unable to receive translation support vulnerable to mistreatment and misdiagnosis. A few of our participants shared that they prioritized accompanying their family members to doctor’s visits to ensure that their family members’ needs are met and that all necessary information is shared between doctor and patient. For those who are not supported in this way, doctor’s visits are oftentimes extremely traumatic rather than restorative.
Outside of their own negative experiences with doctors, our participants shared that they experience secondary trauma from the medical experiences of other Black women and femmes. Namely, several of our interviewees shared that they are still impacted by the fact that Serena Williams nearly died from a pulmonary embolism during childbirth. While many have heard similar stories of maternal mortality in their communities, through hearing that a wealthy, high-profile celebrity experienced similar complications they are forced to reckon with the fact that they cannot buy their way out of a system that is entrenched with anti-Blackness. Certainly, the secondary trauma does not have to come from the experience of a celebrity. Some shared that while they have had positive experiences with doctors, they have watched their loved ones suffer in medical institutions and have had to intervene on their behalf.
The majority of participants who had positive experiences with medical practitioners shared that they have seen the same doctor since they were a child. Through developing this long-term relationship, they were able to build trust and understanding with their provider. However, we recognize that there are several factors that would prevent people from sticking with the same provider including relocation, change of health insurance, and a change in medical needs. Additionally, a potential downside of having the same doctor since childhood is that it may be hard to assess the quality of care that is being received. Consequently, some participants who had this experience shared that their experiences were “neither good nor bad.”
A few of our participants were either medical students themselves, or they had parents who were doctors. Understandably, these individuals demonstrated greater comfort in navigating the medical system than others. Conversely, some of our participants who described their experiences with doctors as “good” did so simply because they did not have access to doctors at all before moving to the United States. Similarly, others who, after lacking health insurance, recently became insured described their current experiences as “good” because, to them, something is better than nothing. These answers show how past experiences can color our perspectives on present treatment which can potentially lead us to tolerate great injustice.
Similar to the situation with therapists, our participants shared that they have a preference for Black doctors. While the doctor’s race does not absolve them of the ability to cause harm, our participants shared that they feel more comfortable, and are more likely to trust a Black doctor. A major way that doctors harm their patients is through fatphobia, which leads them to misdiagnose and mistreat Black women and femmes based on flawed assumptions. Consequently, it is alarmingly clear that unless doctors do the work to dismantle fatphobia as well as transphobia, misogynoir, ageism, and other forms of prejudice, Black women and femmes will not be safe in their presence.
Although our research was centered on people who are not detained, it is also necessary to highlight that medical violence also occurs in detention centers and throughout the carceral system. In September 2020, Dawn Wooten, a nurse working in Irwin Detention Center, revealed that immigrants were being forced to have hysterectomies.16 The news forced us to contend with how, throughout history, Black bodies have been experimented on and mutilated in the name of medicine. Consequently, in order for harm to be reduced in the field of medicine, the foundation of it needs to be assessed, questioned, dismantled and re-imagined.
Self-care
CONTENT WARNING: colorism
FIRST THINGS FIRST I allow myself to dress my soul the way I want to…you know what I’m saying? Like I said, I told people when I’m dressed up…I’m not just in this body…I’m dressing my soul.
The majority of our participants shared that they practice self-care. This finding affirms the fact that, despite all of the responsibilities that Black immigrant women and femmes have, they are still proactively trying to center their health and wellbeing. The few that did not practice self-care shared that they were unable to due to work, school and other responsibilities. Ultimately, time was their biggest obstacle.
Do you practice self-care?
The image shown breaks down the percentage of Black immigrant women and femmes that practice self-care and those who do not. The majority (95.2%) stated that they do practice self-care. 4.8% stated that they do not practice self-care.
- Physical self-care: activities done for physical wellbeing such as exercising, eating well and sleeping well
- Emotional self-care: activities done to find outlets for our feelings such as talking to a therapist, listening to music and journaling
- Spiritual self-care: exploring and expressing our beliefs, morals and values such as prayer, reading scripture or being in nature
- Intellectual self-care: finding ways to practice critical-thinking, grow knowledge and stimulate the mind
- Social self-care: nurturing relationships outside of family, which includes friendships, relationships with neighbors, and so on
- Relational self-care: strengthening close, familial relationships like the relationship between partners, children and their parents, siblings, and so on
- Safety and security self-care: activities done to stabilize personal, environmental and financial security17
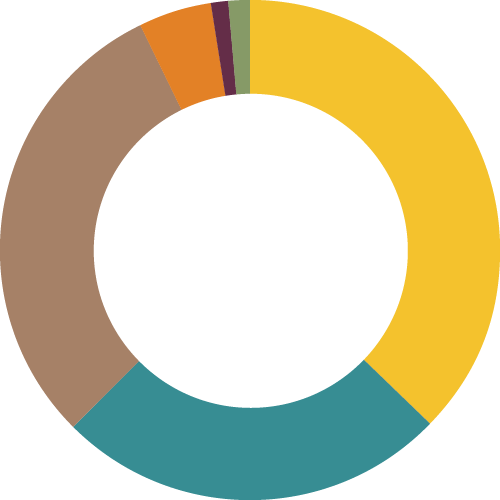
what are your self-care practices?
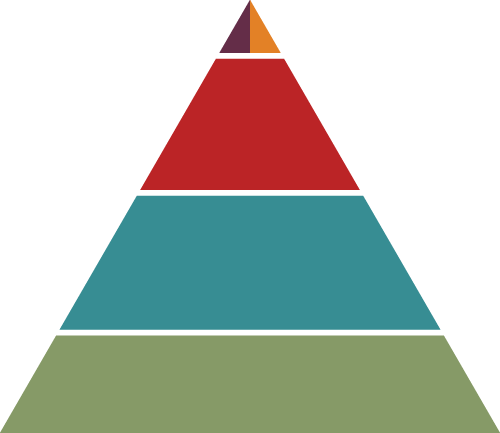
The image shown breaks down the self-care practices of our participants into the categories listed above. In total, there were 263 self-care activities listed. 42.6% of these activities were linked to physical wellbeing. 33.1% of these activities were linked to emotional wellbeing. 8.0% of these activities were linked to relational self-care. 5.3% of these activities were linked to spiritual self-care. 4.9% were linked to social self-care. 1.1% of these activities were linked to safety and security.
It is important to know that we recognize that there is great overlap among between these categories. For example, while speaking to a therapist is classed as emotional self-care it can definitely also be placed in categories such as safety and security.
We find it significant that the leading form of self-care that our participants practiced was physical. This illustrates the degree to which Black immigrant women and femmes prioritize caring for their bodies. Some of the ways that they do this includes going on walks, getting massages, reiki, going shopping and doing their makeup. These activities highlight how important pleasure it is for our liberation.
Additionally, we learned that self-care does not always mean actively doing something, it can also be related to controlling what we passively consume. One of our participants shared the reason why she finds it so important to curate her Instagram feed:
Community-care
CONTENT WARNING: gender-based violence
UM, I THINK WE NEED TO CREATE MORE SAFE SPACES for, um, Black immigrant women and girls to feel comfortable to share about their experiences and to have each other as a support group. So I think, um, what you guys are doing with this research is really great and it will also be even greater to connect with everyone who participated from this to see like how people can serve as like a support system or support group for other people and maybe have recurring workshops or things of that nature.
While self-care is important, we believe that community-care is essential. The assertion that Black immigrant women and femmes always have to take care of themselves reinforces the superhuman stereotype that is violently placed upon us. We need spaces to be soft, vulnerable and to ask for help when necessary.
In our study, we asked our participants to share how their communities can support the mental health of Black immigrant women and femmes. Overwhelming people shared that they simply want to have intergenerational conversations and to truly have their perspectives heard. Specifically, they ask for these spaces to feature frank conversations where the shame and stigma that are associated with mental health can be dismantled. There was a preference for having in-person conversations, but virtual conversations were also suggested.
Our respondents also shared a desire to hold perpetrators of gender-based violence, which overwhelming were named as cis-heterosexual Black men, accountable for the harm they have caused. Cis-heterosexual Black men have to actively work towards combating misogynoir and the responsibility should not fall on women and femmes to teach them how to do that.
Community-based accountability processes and transformative justice will allow Black immigrant women and femmes to feel safer in their communities and to not live in a constant state of fear.
Blueprint for Liberation
While we were interested in the practical things that communities could do to honor and protect Black immigrant women and femmes, we also wanted to dream about what would be possible if finances were not a barrier. We see these dreams as part of a broader blueprint for liberation.
In order to get our participants dreaming, we asked them to share how they would use one million dollars to better the mental health of Black immigrant women and femmes. Here are some of the beautiful, bold and revolutionary visions outlined by our participants:
Maybe cooking classes, maybe just someplace for talk therapy. Just a place to come together and just know that it’s okay if you want to talk, you can, if you don’t want to, you don’t have to. If you want to do art, knitting, writing, reading…just to have a safe place to just be because I know that there are people that, you know, they are in more dire situations where they probably need a shower or warm meal or something. And I’m fortunate that my situation is not like that, but it can be and it is like that for others, so maybe some kind of temporary housing, you know? A place to get feminine supplies when you need it. Take a shower if you don’t have access to it.

We keep us safe and that is in all aspects whether it be physical safety, mental safety, emotional safety, financial safety. We need our own thing. So what I’m talking about is underground therapists,underground like energy workers…like underground priests or mambos or Babalawos…
So it’s like no we need to like let Black people [know Black] is magic like we’re magic. So we need to, we need to tap into the legacy and start an underground railroad. We got like some undocumented folks cause you especially when it just come like they’re going to be go through a lot, they gonna feel a lot. You can’t just leave them by themselves and I hope for the best. Like you need someone that’s going to check in on them. Like we need more doulas. We need more like, like I said, Reiki workers, like all types of aspects that relate to mental health and find a way to figure out how can we cover the funds for their time, you know like and make it free to the people who need it. Like we need to figure that out cause like I think there’s more to life than money. There is more to life than money….I feel like we just need to put our heads together. Yeah. It’s an underground railroad but for mental health called the wellness people or something..like little guardian people.

I have always wanted to open a therapy ice cream truck. Like the concept of someone yearning like following the music because you really want ice cream in the summertime, but you are getting therapy. So, I would make that…I would turn that into a real thing. Maybe we would be giving out plates of rice. I don’t know, but yeah, I think getting people to be comfortable with themselves in this new space that they find themselves in would help.
what I would do is open a lot of Zumba studios, where women could come…not just [for] Zumba, but Zumba dance studios where people could come and explore their sexuality through dance. And actually sit down and just have a conversation in those spaces. Because one thing I realized is that if you connect social space with these conversations, it’s easier for people to open up. Because they’re in these spaces, they’re having fun, and all of a sudden they trust and then you all, you’re not just having fun together, you’re also having these deeper conversations.
I don’t think I’m best suited to plan a project with a million dollars. First, I guess, I would gather a working group of Black health practitioners, so Black woman therapists, Black immigrant therapists, Black Executive Directors of non-profits that address issues around sexual assault, um, Black immigrant lawyers…I’d gather them in a room and have them talk about how they’re going to spend that million dollars. I don’t know much about it because I’m just affected by it, but I had never had to intentionally think about solution making. I don’t think I should. I think there are people who already have ideas and just need money. So give it to those folks. Let them solve the problem.
Everyone has seen Black Panther and now it’s cool to be African, but growing up it wasn’t. It was just like, you’re not Black, and Black people would be like you’re African and it would mean you were dirty, or you lived in huts. And your African parents are telling you that you’re better than the Americans and I was just confused. I feel like we all look the same. I don’t know what’s going on here. And then you get older and you understand history and its nuances. But yeah I feel like just more resources and support for Black Americans and Black immigrant women to come into a space and share their stories and support one another. I feel like that’s how we’re going to grow. We can’t be one against the other.
I think the focus would be having our core…having African American or also immigrant or any ethnic studies as a core requirement in schools…all schools, because we don’t, it’s always seen as an elective. I’m tired of that. Because then history is shown in one way or even painted one way and there’s not the, our story is not shared. So one, I think the story needs to be shared. Two, we need to also start portraying Black women in the media more and not just as the strong Black friend with the sassy attitude…or even the immigrant with broken English. We need to show women in their versatility. Show how multifaceted they are.
So this might be the radical, communal spirit that I have, but I would probably do like a really dramatic you know micro-grant situation you know what I mean. So as many of the sister-friends can see their ideas come to fruition. Whether those are like the singers, the visual artists, or maybe it is the business woman, or maybe it is the doctors or nurses, maybe it is the teachers. But everybody can explore what healing would look like for Black women and girls in their different ways. Because I would struggle “to like have one way, and then it would be like we all have power in deciding and choosing in the multiplicity of our experiences, even though there is a shared identity. We can do this in so many different ways.
Maybe cooking classes, maybe just someplace for talk therapy. Just a place to come together and just know that it’s okay if you want to talk, you can, if you don’t want to, you don’t have to. If you want to do art, knitting, writing, reading…just to have a safe place to just be because I know that there are people that, you know, they are in more dire situations where they probably need a shower or warm meal or something. And I’m fortunate that my situation is not like that, but it can be and it is like that for others, so maybe some kind of temporary housing, you know? A place to get feminine supplies when you need it. Take a shower if you don’t have access to it.
I have always wanted to open a therapy ice cream truck. Like the concept of someone yearning like following the music because you really want ice cream in the summertime, but you are getting therapy. So, I would make that…I would turn that into a real thing. Maybe we would be giving out plates of rice. I don’t know, but yeah, I think getting people to be comfortable with themselves in this new space that they find themselves in would help.
I think the focus would be having our core…having African American or also immigrant or any ethnic studies as a core requirement in schools…all schools, because we don’t, it’s always seen as an elective. I’m tired of that. Because then history is shown in one way or even painted one way and there’s not the, our story is not shared. So one, I think the story needs to be shared. Two, we need to also start portraying Black women in the media more and not just as the strong Black friend with the sassy attitude…or even the immigrant with broken English. We need to show women in their versatility. Show how multifaceted they are.
So this might be the radical, communal spirit that I have, but I would probably do like a really dramatic you know micro-grant situation you know what I mean. So as many of the sister-friends can see their ideas come to fruition. Whether those are like the singers, the visual artists, or maybe it is the business woman, or maybe it is the doctors or nurses, maybe it is the teachers. But everybody can explore what healing would look like for Black women and girls in their different ways. Because I would struggle “to like have one way, and then it would be like we all have power in deciding and choosing in the multiplicity of our experiences, even though there is a shared identity. We can do this in so many different ways.
Recommendations
Policy-Related Recommendations
- Provide universal healthcare that includes immigrants and undocumented people.
- Repeal the Violent Crime Control and Law Enforcement Act of 1994, the largest crime bill in U.S. history, that has led to increased criminalization and incarceration.
- Streamline and enhance the process to apply for public benefits: reduce wait-times and bureaucracy, process all information in one location close to the applicants residency, offer interpretation and expand the criteria for people to enlist in and maintain eligibility for public benefits.
- Provide social service support for Black immigrant women and femmes of all ages, sexualities and abilities (workforce development, educational opportunities, and fund NGOs that support their needs).
- Provide more affordable housing and the government should provide financial assistance for homeownership.
- Increase the minimum wage to a living wage.
- Demand that perpetrators of discrimination, including those who inact violence in professional settings, are held accountable for their actions.
- Streamline the U-visa process more and disallow the police from certifying visas.
- Protect all Black immigrants, regardless of status, which includes DED and TPS holders, DACA, and the other 11 million undocumented folks.
- Restore asylum and refugee resettlement.
- Mandate a complete separation between health professionals and law enforcement agencies like ICE, police and sheriffs.
- Actualize sanctuary cities.
Community-Based Recommendations
- Believe people when they share accounts of the violence they have experienced. Protect them and honor them by centering their experiences in accountability processes that are aligned with their ideas of justice.
- Assist perpetrators of gender-based violence in holding themselves accountable for the harm they have caused. The responsibility to make this happen should not be placed on survivors.
- Expand holistic, long-term trainings on intimate partner violence to deeply analyze and combat the different forms of emotional abuse including gaslighting.
- Create, promote and distribute mental health resources throughout our communities. Ensure that these resources are translated into a variety of languages and formats to ensure that the information is truly accessible.
- Provide free or affordable culturally competent therapy to Black immigrant women and femmes over a sustained period of time.
- Train faith leaders on mental health and wellness and encourage them to promote this knowledge to their congregations/members. Mandate that faith leaders assist perpetrators of gender-based violence in holding themselves accountable and that faith leaders hold themselves accountable if they themselves are a perpetrator.
- Support participatory research on the mental health of Black immigrant transwomen and non-binary people.
- Create more spaces and dialogues where Black people can have in-house conversations to further their political education and to build deeper relationships with one another. These spaces should be inclusive of transwomen and non-binary people.
Transparency
LIMITATIONS OF THE STUDY
At BAJI, we believe that all research should facilitate learning and growth not only for the audience that encounters the project, but for the researchers themselves. While we are extremely proud of this report, we want to invite you into the process of examining its limitations. Admittedly, many of our limitations are a product of the finite funds and time-constraints that are commonplace when working within the non-profit industrial complex. We hope that by making this process communal, we can strengthen not only our research going forward, but yours too. While the list below details some of the major limitations of our research, it is by no means exhaustive.
Major limitations:
- The report lacks gender diversity as the majority of our participants identified as cis-gender women.
- The majority of our participants were recruited by BAJI’s staff/research fellows, which could have lead to a participation bias.
- While the age range for our report is expansive (18-84), the representation of elders is small.
- Given that our research fellows were based in major cities, the report lacks representation of people who live in rural areas.
- Additionally, we wish that we could have met the needs of our participants and researchers given how much they shared of themselves to make this study possible. Some of these needs included therapy, housing, and citizenship.
ACCOUNTABILITY AT BAJI: CENTERING SURVIVORS
During the writing of this report, several Black women and femmes came out and shared that they experienced emotional abuse and sexual predation at the hands of a BAJI staffer. Additionally, they shared that this abuse was enabled by another BAJI staffer. While both staffers who were mentioned were not a part of this study, it is important for us to be transparent about the context in which this report was created. In order for the recommendations that we provide in this report to be sincere, we must be introspective and commit to the continuous work of dismantling patriarchy and all forms of gender-based violence. As of July 2020, we have begun internal and external transformative justice processes to address the harm caused and to facilitate healing. Above all, we will continue to center and believe the survivors who have come forward just as we believe the survivors who shared their stories in this report.
Conclusion
This report demonstrates the ingenuity, resilience and power of Black immigrant women and femmes while also detailing the trauma and hardships they are made to carry. It is through such holistic depictions that we can truly come to understand the fullness of the experiences that Black immigrants have in the U.S. and how these experiences impact their physical, mental and spiritual health. This report demonstrates that interactions with the police, ICE, healthcare practitioners, benefits administrators, and other agencies and officials can lead to negative health outcomes for Black immigrants. Consequently, we do not only believe in the importance of therapy, but also in the abolition of all forms of policing. We uplift the sentiments of our participants who shared that therapy is most beneficial when the therapist is Black, culturally-competent, and affirms their gender and sexuality. We believe that advocating for the wellness of individuals cannot occur outside of advocating for wellness for families and entire communities. Above all, we believe that therapy, like medical care, housing, education, and other needs, should be free and accessible to everyone.
This report simply scratches the surface of the mental health of Black migrants in the U.S. Consequently, we encourage others to continue this investigation so that we can continue to uplift our people’s stories. Specifically, we ask you to join in our committment to centering the mental health of Black transgender and non-binary people. This report demonstrates the importance of paying attention and catering to the mental wellness of Black immigrants in prisons and detention centers. Importantly, we encourage those that engage in this kind of research to compensate participants for their time, ensure their data is confidential, and provide them with mental health support or, at the very least, resources to support their needs.
At BAJI, we do not believe in research for research sake. We are committed to using this research to push for policy change, to advance our organizing strategies and to inform how we engage with our communities. We also believe that you, the reader, are a critical part of our research process. We would love to engage you in our gender justice work, answer any questions that you may have, and build with you. To reach out to us, email: genderjustice@baji.org.
Most importantly, we want to sincerely thank our 84 interviewees for being vulnerable with us and for trusting us with their stories. This report would have been impossible without them. We will strive to honor what they have shared with us by fighting for the liberation of Black immigrant women and femmes, always.
Resources
ORGANIZATIONS/INITIATIVES/WEBSITES
- Black Dream Escape
- The Black Emotional and Mental Health Collective (BEAM)
- Black Girl in Om
- Black Girls Breathing
- Black Girls Smile
- Black LGBTQIA+ Migrant Project (BLMP)
- Black Women for Wellness
- Ethel’s Club
- Healing While Black LLC
- Interrupting Criminalization
- Justice Teams Network: Alternatives to Police in Mental Health Response Campaign
- The Homecoming Podcast by Dr. Thema Bryant
- The Loveland Foundation
- The Nap Ministry
- The National Queer and Trans Therapists of Color Network (NQTTCN)
- The Steve Fund
- Therapy for Black Girls
- Transform Harm
NATIONAL HELPLINES
Trans Lifeline
Phone: 877-565-8860
Hours of Operation: 24/7/365
Trans Lifeline is a grassroots hotline and microgrants 501(c)(3) non-profit organization offering direct emotional and financial support to trans people in crisis – for the trans community, by the trans community.
The Trevor Project
Phone: 866-488- 7386
Hours of Operation: 24/7/365
Founded in 1998 by the creators of the Academy Award®-winning short film TREVOR, The Trevor Project is the leading national organization providing crisis intervention and suicide prevention services to lesbian, gay, bisexual, transgender, queer & questioning (LGBTQ) young people under 25.
HELPLINES IN NYC
National Alliance on Mental Illness of New York City
Phone: (212) -684 -3264
Hours of Operation: M-F 11am to 6pm
The helpline allows you to:
- Find help navigating NYC’s mental health system from people with personal experience
- Receive referrals for mental health services, housing, legal assistance and more.
- Learn about NAMI NYC classes, support groups, events and other support programs.
New York City Lifenet
Phone: 800-LIFENET
Hours of Operation: 24/7
A free, confidential helpline for New York City residents. The hotline’s staff of trained mental health professionals help callers find mental health and substance abuse services.
NYC Well
Phone: 1-888-NYC-Well
Text: WELL to 65173
Chat: speak to a counselor at nyc.gov/nycwell
Hours of Operation: 24/7/365
NYC Well is a one-click, one-call connection to counseling, crisis intervention, peer support, and referrals to ongoing treatment and support services. NYC Well is free, 24/7/365 confidential mental health support for all New Yorkers. This toll-free, multilingual, crisis support service is available in English, Spanish, and Mandarin/Cantonese, with translation available in more than 200 languages.
HELPLINES IN MIAMI
Banyan Health Systems 24-Hour Crisis Hotline
Phone: 305-774-3616
Hours of Operation: 24 hours a
day/7 days a week
Suicide Prevention/SAFENET
Phone: 305-358-4357
Miami-Dade Advocates for Victims/Safespace North and South Hotline
Phone: 305-758-2546
Domestic Violence Hotline
Phone: 800-962-2873
HELPLINES IN MINNESOTA
Abbott Northwestern Hospital
Phone: 612-863-8633
Experts at this hospital are available to respond to people experiencing a crisis or an emotional, stressful situation
Domestic Violence Abuse Service Center (DASC) Line for Counselling and Shelter
Phone: 866-223-1111
Hours of Operation: 24 hours a day/7 days a week
First Call for Help
Phone: 211
This database connects callers with resources such as grief support, housing and mental health services
Hennepin County Medical Center Suicide Hotline
Phone: 612-873-2222
Hennepin County Medical Center Crisis Referral Line
Phone: 612-873-3161
HELPLINES IN LA
ACCESS-LA County Helpline
Phone: 1-800-854-7771
Hours of Operation: 24 hours a day/7 days a week
Provides linkages to consumers to mental health services in the community & resources to consumers in crisis.
CA Youth Crisis Line
Phone: 1-800-843-5200
The statewide emergency response system for youth (ages 12-24) and families in crisis. It has access to more than 5,500 free or low-cost resources for youth and families across CA.
LA Warmline
Phone: 1-855-952-WARM (1-855-952-9276)
Hours of Operation: 10pm – 6am
A confidential overnight telephone support service in English & Spanish for anyone in Southern California who is struggling with loneliness, anxiety, substance use, mental health concerns, or needs information about available mental health services.
Project Return Warm Line
Phone: 1-888-448-9777/1-888-448-4055 (Spanish)
Hours of Operation: M – F, 5pm – 10pm & Sat, 11am – 4pm
Works Cited
Akinsulure-Smith, A. M. (2016). Resilience in the Face of Adversity: African Immigrants’ Mental Health Needs and the American Transition. Journal of Immigrant & Refugee Studies, 428–448. https://doi.org/10.1080/15562948.2016.1238989
Alegría, M., Álvarez, K., & DiMarzio, K. (2017). Immigration and Mental Health. Current Epidemiology Reports, 4(2), 145–155. https://doi.org/10.1007/s40471-017-0111-2
Anderson, M. (2020, May 30). Statistical Portrait of the U.S. Black Immigrant Population. Pew Research Center (Report). Retrieved August 27, 2020, from https://www.pewsocialtrends.org/2015/04/09/chapter-1-statistical-portrait-of-the-u-s-black-immigrant-population
The Black Women’s Truth & Reconciliation Commission (Report.) (2016) Black Women’s Blueprint. https://www.bwbtraining.org/the-truth-and-reconciliation
Tanis, F. & C., & Brown, S., The Sexual Abuse to Maternal Morality Pipeline. (Report). Black Women’s Blueprint. (2019). https://drive.google.com/file/d/1S3qcOb0oCvYcAjttaldgwbH_ErwovSzd/view
Famn Saj. (2018). Sacred Healing Circles: Narrative Power Report (Brochure).
https://www.fanmsaj.org/
Gunn, D. (2019, February 26). Non-White School Districts Get $23 Billion Less Funding Than White Ones. Pacific Standard. Retrieved August 27, 2020, from https://psmag.com/education/nonwhite-school-districts-get-23-billion-less-funding-than-white-ones
Hoffman, K. M., Trawalter, S., Axt, J. R., & Oliver, M. N. (2016). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proceedings of the National Academy of Sciences of the United States of America, 113(16), 4296–4301. https://doi.org/10.1073/pnas.1516047113
Kiana Davis, Helen Strom, Craig Hughes, and Zak Aldridge. The Bureaucracy of Benefits: Struggling to Access Public Assistance and SNAP in New York City. (Report.) Safety Net Project and Safety Net Activists at the Urban Justice Center. January 2019.
Marks AK, Ejesi K, García Coll C. Understanding the US immigrant paradox in childhood and adolescence. Child Development Perspectives. 2014;8(2):59.
Nonko, E. (2018, March 26). Nearly 250,000 NYC rental apartments sit vacant. 6sqft, Retrieved August 27, 2020, from https://www.6sqft.com/nearly-250000-nyc-rental-apartments-sit-vacant/
Scribner R. (1996). Paradox as paradigm–the health outcomes of Mexican Americans. American Journal of Public Health, 86(3), 303–305. https://doi.org/10.2105/ajph.86.3.303
Treisman, R. (2020, September 16). Whistleblower Alleges ‘Medical Neglect,’ Questionable Hysterectomies Of ICE Detainees. NPR. Retrieved October 11, 2020, from https://www.npr.org/2020/09/16/913398383/whistleblower-alleges-medical-neglect-questionable-hysterectomies-of-ice-detaine
Williams-Nickelson, C. (2006). Balanced Living Through Self-Care. In J. Worell & C. D. Goodheart (Eds.), Oxford series in clinical psychology. Handbook of girls’ and women’s psychological health: Gender and well-being across the lifespan (p. 183–191). Oxford University Press.
Appendix
Keywords
Keywords
While the words and phrases listed here have multiple meanings, the definitions that you see are a reflection of the ways in which we are using said terms within the scope of this report. We also recognize that language is always evolving. If the meanings of any of the words that we use becomes derogatory by the time you encounter this report, we apologize for unintended harm caused. We are continuously committed to updating the language that we use to affirm and respect our collective communities.
- Acculturation hypothesis: a phenomenon supported by research which indicates that the longer immigrants stay in the U.S., the more their mental health declines
- Ageism: prejudice or discrimination on the grounds of a persons age
- Anxiety: a mental health disorder characterized by feelings of worry or fear that are strong enough to interfere with one's daily activities
- Art Therapy: involves the use of creative techniques such as drawing, painting, collage, coloring or sculpting to help people express themselves artistically and examine the the psychological and emotional undertones in their art
- Asexual: a person who experiences a lack of sexual attraction to others, or low or absent interest in or desire for sexual activity
- Assimilation: the process by which a person or a group's language and/or culture comes to resemble those of another group
- Black immigrants: Black people who self-identify as being immigrants due to either their migration or the migration of their parent(s), or grandparent(s)
- Cis-gender: denoting a person whose identity and gender corresponds with the sex they were assigned at birth
- Code-switch: adjusting one's speech, appearance, behavior and expression in ways that will optimize the comfort of others in exchange for fair treatment, quality service, and employment opportunities
- Cognitive Behavioral Therapy: focuses on challenging and changing unhelpful cognitive distortions and behaviors, improving emotional regulation, and the development of personal coping strategies that target solving current problems
- Content warning: are verbal or written notices that precede potentially sensitive content
- Crystal Therapy: an alternative medicine technique that uses stones and crystals for healing
- Depression: a mood disorder that causes a persistent feeling of sadness and loss of interest and can interfere with your daily functioning
- Dyslexia: a learning disorder that involves difficulty reading
- Emotional self-care: activities done to find outlets for your feelings such as talking to a therapist, listening to music and journaling
- Fatphobia: a system of structural oppression and violence towards fat people or people whose bodies do not conform to social expectations of physical size
- Femme: A gender expression or identity that queers or subverts femininity, but is not tied to the category of womanhood. E.g.— People who identify themselves as femme may also identify as non-binary, trans, cis, women, men and/or any other gender.
- Gaslighting: manipulating someone by psychological means into questioning their own sanity
- Homogenize: make uniform or singular
- Individualistic: characterized by being self-reliant and independent
- Intellectual self-care: finding ways to practice critical-thinking, grow knowledge and stimulate the mind
- Intergenerational trauma: is a psychological term which asserts that trauma can be passed down between generations
- LGBTQ+: refers to individuals who are lesbian, gay, bisexual, transgender, queer and others.
- Maternal mortality: the death of a person while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management but not from accidental or incidental causes
- Mindfulness-based Cognitive Therapy: is an approach to psychotherapy that uses cognitive behavioral therapy methods in collaboration with mindfulness meditative practices and similar psychological strategies
- Misogynoir: hatred, dislike, distrust and prejudice directed towards Black women
- Non-binary: relating to people whose gender identity is more expansive than the binary of male or female. Many, but not all, non-binary people identify as transgender.
- Non-citizen(s): non-citizen refers to people born outside the U.S. Puerto Rico or other U.S. territories, excluding people who are U.S. citizens
- Non-profit industrial complex: is a system of relationships between, the State (or local and federal governments), the owning classes, foundations, and non-profit/NGO social services and social justice organizations that results in surveillance, control, derailment, and everyday management of political movements
- Open-ended question: allowing the formulation of any answer, rather than a selection from a set of possible answers
- Participation bias: is a phenomenon in which the results of elections, studies, polls, etc. become non-representative because the participants disproportionately possess certain traits which affect the outcome
- Physical self-care: activities done for physical wellbeing such as exercising, eating well and sleeping well
- Public Assistance (PA): refers to assistance programs that provide either cash assistance or in-kind benefits to individuals and families from any governmental entity. There are two major types of public assistance programs; social welfare programs and social insurance programs. Examples of public assistance include Medicaid, food stamps and housing assistance
- Pulmonary embolism: is a blockage of an artery in the lungs by a substance that has moved from elsewhere in the body through the bloodstream
- Reiki: a healing technique based on the principle that the therapist can channel energy into the patient by means of touch, to activate the natural healing processes of the patient's body and restore physical and emotional well-being
- Relational self-care: strengthening close, familial relationships like the relationship between partners, children and their parents, siblings, and so on
- Remittances: a sum of money sent, especially by mail, in payment for goods or services or as a gift
- Safety and security self-care: activities done to stabilize personal, environmental and financial security
- School-to-prison pipeline: refers to the processes through which children, who are disproportionately Black and brown, are funnelled out of schools and into the juvenile and criminal justice system
- Sciatica: a pain that radiates along the path of the sciatic nerve, which branches through your lower back through your hips and buttocks and down each leg
- Secondary trauma: is defined as indirect exposure to trauma through a firsthand account or narrative of a traumatic event
- Self-care: is any activity that we do deliberately in order to take care of our mental, emotional and physical health
- Sexual assault: is an act in which a person intentionally sexually touches another person without that person's consent, or coerces or physically forces a person to engage in a sexual act against their will
- Sexual harassment: behavior characterized by the making of unwelcome and inappropriate sexual remarks or physical advances in a workplace or other professional or social situation
- Sickle cell anemia: a blood disorder that results in an abnormality in the oxygen-carrying protein haemoglobin found in red blood cells
- Snowball sampling: is where research participants recruit other participants for a test or study
- Social self-care: nurturing relationships outside of family, which includes friendships, relationships with neighbors, and so on
- Spiritual self-care: exploring and expressing our beliefs, morals and values such as prayer, reading scripture or being in nature
- Stigma: a mark of disgrace associated with a particular circumstance, quality or person
- Supplemental Nutrition Assistance Program (SNAP): the largest federal nutrition assistance program
- Support system: a network of people who provide an individual with emotional or practical support
- Transgender: relating to people whose gender does not correspond with the sex they were assigned at birth
- Transphobia: a system of structural oppression and violence towards transgender people or people who do not conform to the gender binary
- Undocumented: a foreign born individual who does not have the legal right to be in or remain in the U.S.
- Weaponized: adapted for use as a weapon
- Weathering: toxic stress resulting from racism, bias and discrimination
- Xenophobia: dislike or prejudice of people from other countries
Questionnaire
Questionnaire
- How did you find out about this research project?
- How old are you?
- Are you employed?
- If so: What is your occupation?
- What are your pronouns?
- Do you have any disabilities that you would be comfortable disclosing to us? Disabilities are physical or mental conditions that limit a person’s movements, senses, or activities. They include disorders, illnesses, diseases and so on.
- How would you describe your gender and sexuality?
- Are you in a romantic relationship?
- If yes: How do you feel about your relationship?
- If no: How do you feel about being single?
- Do you have children?
- If so: How many?
- What is your ethnic background — where is your family from?
- Were you born in the United States or elsewhere? If elsewhere, please state the country.
- If born elsewhere: How old were you when you migrated to the U.S.?
- If born elsewhere: How long have you lived in the U.S.?
- Do you have family who live in your home country?
- *If no: Skip follow up questions and go to 12*
- If so: How are they doing — are there any struggles that they are currently experiencing?
- If family isn’t doing good: Some immigrants do not talk about mental health because they believe their issues are small in comparison to the challenges that people back home are facing. Do you feel this way?
- If family is doing good: What are the factors — be they financial, political, or emotional — that you believe contributes to your family’s happiness back home?
- What are your responsibilities in terms of your family? Responsibilities could include supporting a family member financially, emotionally, in prison or detention or otherwise.
- How are you doing in the United States — are there any struggles you are currently experiencing ?
- If they are doing good: What are the factors — be they financial, political, or emotional — that you believe contributes to your happiness here?
- If you migrated to the U.S., did you have expectations before you moved?
- If yes: What were your expectations of the U.S.?
- If yes: Has your experience matched your expectations?
- Do you have any needs at the moment? This could include things like food, housing, work, clothing etc.
- Do you use any government benefits such as Medicaid, food stamps, public housing, or welfare?
- If so: Which ones do you use and what has been your experience in trying to use these resources?
- Do you identify with a particular religion/spiritual practice? If so, which one (s)?
- *If no: Skip the questions below and go to 18*
- If yes: Does your religion/spiritual practice have positive or negative consequences on your mental health?
- Is this the same religion/spiritual practice that you were raised under?
- If no: Where did you first learn about the religion/spiritual practices that you now observe?
- Do you feel that your place of worship can understand and address the challenges Black immigrant women and femmes face?
- In your community, what are the attitudes towards the religion/spiritual practice that you currently engage in?
- Self-care is any activity that we do deliberately in order to take care of our mental, emotional and/or physical health. Do you practice self-care?
- If yes: What do you do?
- If no: Why don’t you? Do you think there are unique experiences and challenges Black immigrant women and femmes face that impact their mental health? This may include challenges in the workplace, interactions with law enforcement and immigration authorities or even personal traumas.
- If yes: How do these experiences affect your mental health?
- How does it make you feel when you hear about ICE raids, detention centers, deportations and anti-immigrant rhetoric, or policies?
- For this question we are going to ask about personal trauma. Have you experienced sexual assault or sexual harrassment? Sexual assault is an act in which a person intentionally sexually touches another person without that person’s consent, or coerces or physically forces a person to engage in a sexual act against their will. Sexual harassment is any sort of unwelcome and inappropriate sexual remarks or physical advances in your neighborhood, workplace or other professional or social situation.
- Have you ever gone to counseling/therapy?
- If yes: How did you find your therapist?
- What was your experience like?
- In your therapy sessions, do you feel that the challenges you shared as a Black immigrant woman/femme were fully understood and addressed?
- If no: Is there a reason why you have not gone to therapy?
- For both yes and no responses: Do you feel like there are boundaries preventing Black immigrant women and femmes from accessing therapy?
- If yes: How did you find your therapist?
- What have your experiences been like interacting with medical practitioners which could include, but are not limited to, primary care physicians, gynecologists, midwives etc. Have you been satisfied with the medical care that you have received in the U.S?
- What were your parents/caregivers attitudes towards mental health when you were growing up and what are they now?
- A support system is a network of people who provide an individual with practical or emotional support. Do you have a support system?
- If so: How would you rate it?
- Very Strong
- Strong
- Neither Strong nor Weak
- Weak
- Very Weak
- Is this rating similar or different to how you would have rated your support system in your home country?
- If no difference: Skip to question 26.
- If different, how would they rate their support system in their home country?
- Very Strong
- Strong
- Neither Strong nor Weak
- Weak
- Very Weak
- If so: How would you rate it?
- Do you have a place that you visit to be around other Black immigrant women/femmes?
- If no: Skip to question 27.
- If so: Where is it?
- How often do you attend these kinds of spaces?
- Very often
- Often
- Sometimes
- Rarely
- Never
- How do these gatherings impact your mental health? What joy do you get out of these experiences? What are the emotional/spiritual benefits of these spaces?
- What do you think can be done to improve the mental health of Black immigrant women/femmes in the United States?
- How can people in your community come together to support the mental health of Black immigrant women/femmes?
- How would you use $1 million to support the mental health of Black immigrant women/femmes?
End Notes
End Notes
- Scribner R. (1996). Paradox as paradigm–the health outcomes of Mexican Americans. American Journal of Public Health, 86(3), 303–305. https://doi.org/10.2105/ajph.86.3.303
- Marks AK, Ejesi K, García Coll C. Understanding the US immigrant paradox in childhood and adolescence. Child Development Perspectives. 2014;8(2):59.
- Breslau, J., Borges, G., Hagar, Y., Tancredi, D., & Gilman, S. (2009). Immigration to the USA and risk for mood and anxiety disorders: variation by origin and age at immigration. Psychological medicine, 39(7), 1117–1127. https://doi.org/10.1017/S0033291708004698
- Black Women’s Blueprint. (2019). The Sexual Abuse to Maternal Mortality Pipeline. https://drive.google.com/file/d/1S3qcOb0oCvYcAjttaldgwbH_ErwovSzd/view
- Ibid.
- Akinsulure-Smith, A. M. (2016). Resilience in the Face of Adversity: African Immigrants’ Mental Health Needs and the American Transition. Journal of Immigrant & Refugee Studies, 428–448. https://doi.org/10.1080/15562948.2016.1238989
- Famn Saj. (2018). Sacred Healing Circles: Narrative Power Report (Brochure). https://www.fanmsaj.org/
- Kiana Davis, Helen Strom, Craig Hughes, and Zak Aldridge. The Bureaucracy of Benefits: Struggling to Access Public Assistance and SNAP in New York City. Safety Net Project and Safety Net Activists at the Urban Justice Center. January 2019.
- Nonko, E. (2018, March 26). Nearly 250,000 NYC rental apartments sit vacant. 6sqft, Retrieved August 27, 2020, from https://www.6sqft.com/nearly-250000-nyc-rental-apartments-sit-vacant/
- Anderson, M. (2020, May 30). Statistical Portrait of the U.S. Black Immigrant Population. Pew Research Center (Report). Retrieved August 27, 2020, from https://www.pewsocialtrends.org/2015/04/09/chapter-1-statistical-portrait-of-the-u-s-black-immigrant-population
- Ibid.
- Gunn, D. (2019, February 26). Non-White School Districts Get $23 Billion Less Funding Than White Ones. Pacific Standard. Retrieved August 27, 2020, from https://psmag.com/education/nonwhite-school-districts-get-23-billion-less-funding-than-white-ones
- Black Women’s Blueprint. (2016). The Black Women’s Truth & Reconciliation Commission (Report). https://www.bwbtraining.org/the-truth-and-reconciliation
- Ibid.
- Hoffman, K. M., Trawalter, S., Axt, J. R., & Oliver, M. N. (2016). Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proceedings of the National Academy of Sciences of the United States of America, 113(16), 4296–4301. https://doi.org/10.1073/pnas.1516047113
- Treisman, R. (2020, September 16). Whistleblower Alleges ‘Medical Neglect,’ Questionable Hysterectomies Of ICE Detainees. Retrieved October 11, 2020, from https://www.npr.org/2020/09/16/913398383/whistleblower-alleges-medical-neglect-questionable-hysterectomies-of-ice-detaine
- Williams-Nickelson, C. (2006). Balanced Living Through Self-Care. In J. Worell & C. D. Goodheart (Eds.), Oxford series in clinical psychology. Handbook of girls’ and women’s psychological health: Gender and well-being across the lifespan (p. 183–191). Oxford University Press.
© 2021 CATHERINE LABIRAN & BLACK ALLIANCE FOR JUST IMMIGRATION
DESIGN BY DUENDE
MAPS USED IN DEMOGRAPHICS SECTION ARE FROM VEMAPS.COM AND FREEVECTORFLAGS.COM